Summary
While a DIEP flap uses the front of the abdomen to provide sufficient volume for breast reconstruction in most women, the SHAEP flap is an excellent option for thin women with fuller breasts. When DIEP flaps alone do not provide sufficient tissue for the reconstruction of both breasts, additional tissue from the “love handle” area on each side can extend the amount of tissue available.
Since the blood supply to the lower abdominal and hip tissue can vary, a preoperative CT angiogram can help identify the perforator blood vessels that are best in any given patient. This can help with surgical planning and can determine how the SHAEP flap will be done.
Types of procedures
- DIEP flap and DCIA flap: The deep circumflex iliac artery (DCIA) provides blood supply to the hip area and is most commonly used in addition to the DIEP flap.
- DIEP flap and SIEA flap: The superficial inferior epigastric artery (SIEA) may also provide blood supply to the hip area and can be used in addition to the DIEP flap.
- DIEP flap and SCIA flap: Alternatively the superficial circumflex iliac artery (SCIA) provides blood supply to the hip area and is used in addition to the DIEP flap.
Procedure details
- CT angiogram before surgery identifies the blood supply
- The surgeon elevates a flap of skin and fat from the front of the abdomen and from the adjacent hips
- Careful microsurgical technique allows exposure of the perforator vessels that feed into the overlying flaps
- The flaps are transferred to the mastectomy defect with the tissue from each side of the abdomen and from each hip being used for each breast
- Blood vessels from the flaps are connected to blood vessels in the chest using the operating microscope
- Having two stacked flaps for each reconstructed breast allows for an adequate volume and shape even in thin patients
- After flap transfer, any incisions in the abdomen and lower waist are closed, much like an extended tummy tuck
Risks & Benefits
As with any free flap breast reconstruction procedure, the SHAEP flap carries a small risk of failure if there is disruption of blood flow to the flap after surgery. This risk depends in part on the level of experience of the plastic surgeon. The surgeons at NYBRA Plastic Surgery are experts in advanced microvascular breast reconstruction and routinely perform such reconstructions with a success rate of greater than 99%.
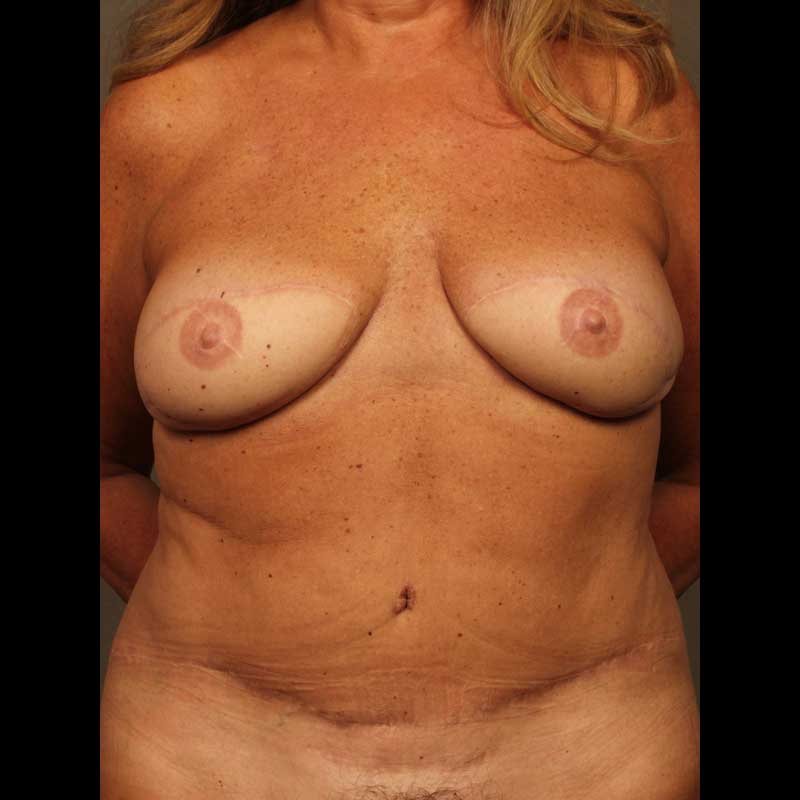
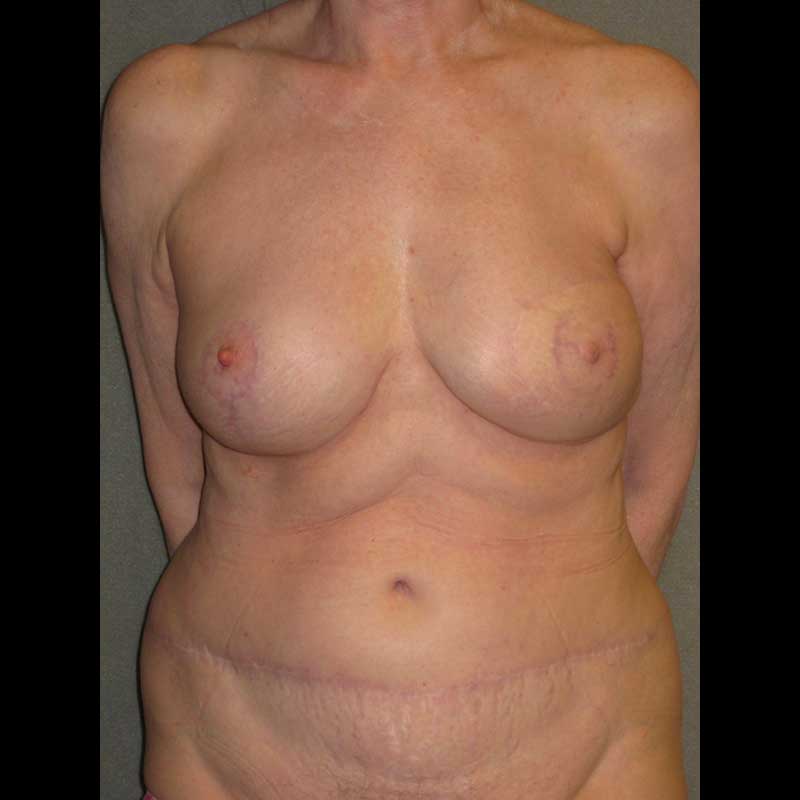
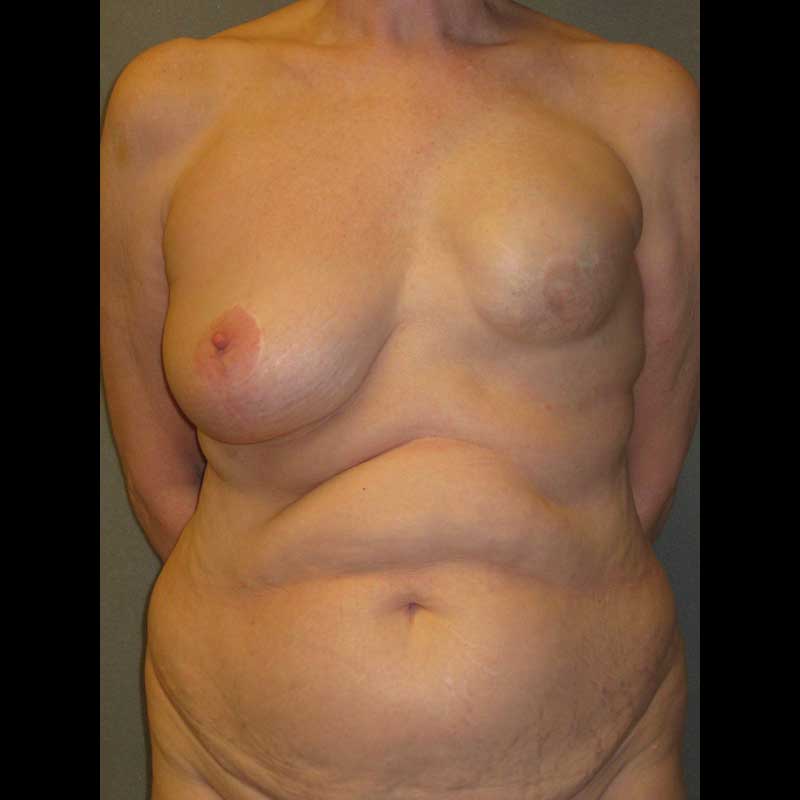
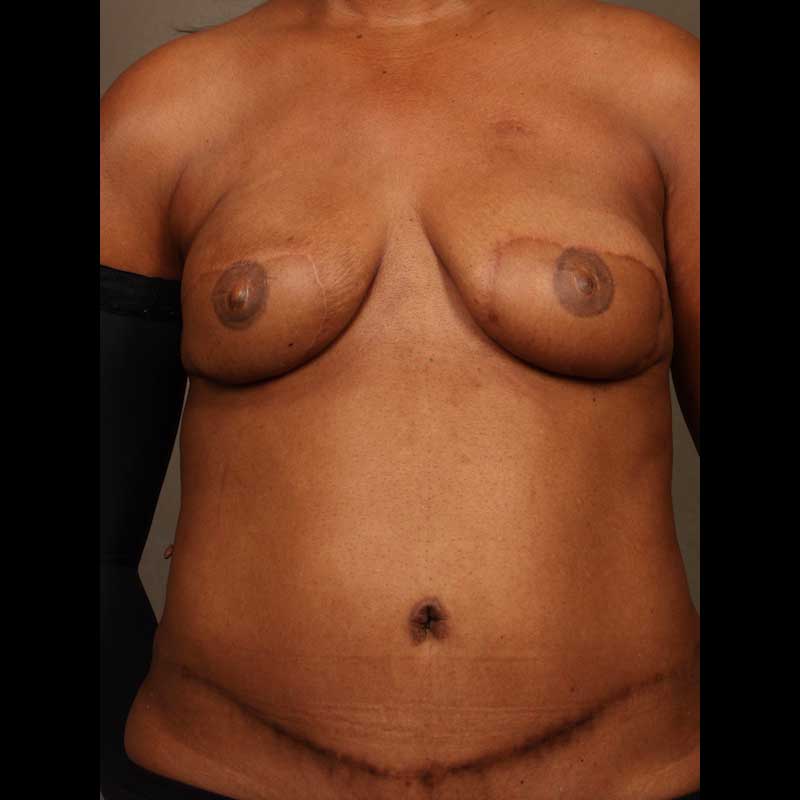
Since tissue from each “love-handle” area is used along with the front of the abdomen, the SHAEP flap often results in a favorable contour with an improved waist line.
Frequently Asked Questions
If the SHAEP flap involves two flaps for each breast, will my recovery be more difficult?
Since all the tissue is taken from the abdomen, the recovery time for the SHAEP flap is similar to the recovery following DIEP flap breast reconstruction. Compared to the DIEP flap the abdominal scar extends further to the sides.