Summary
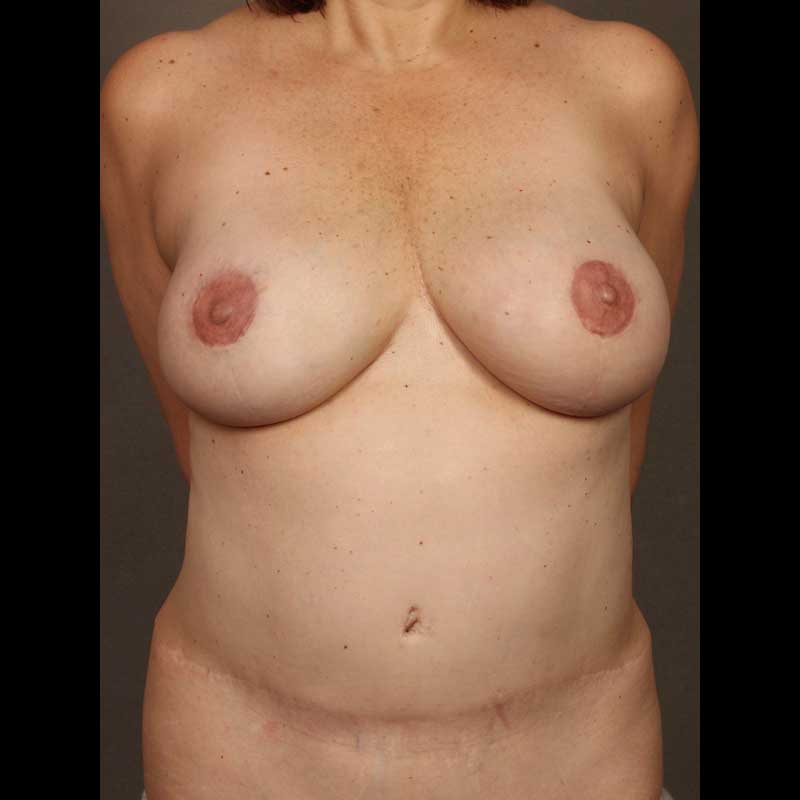
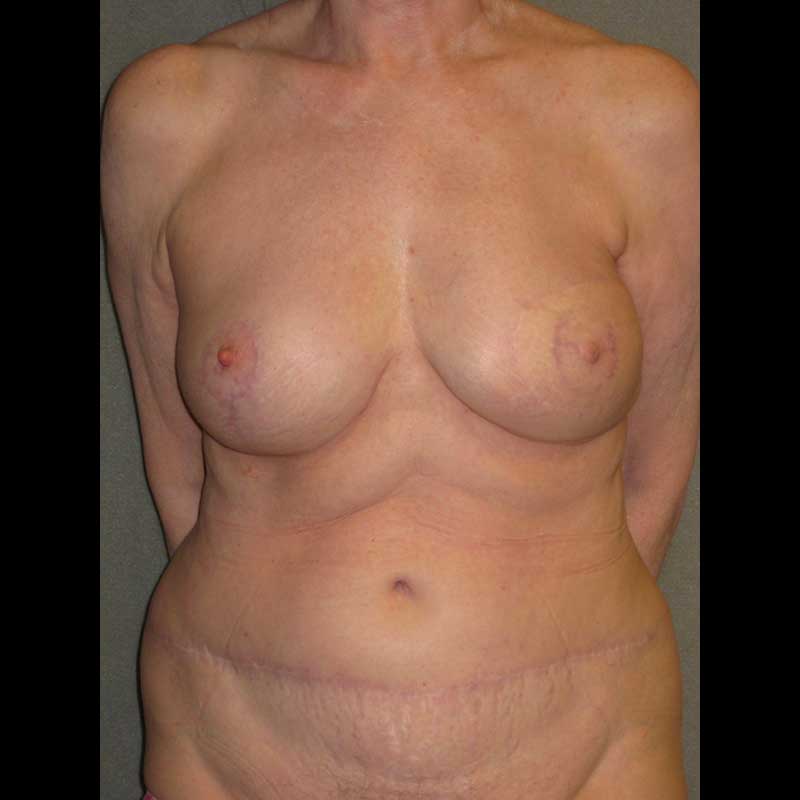
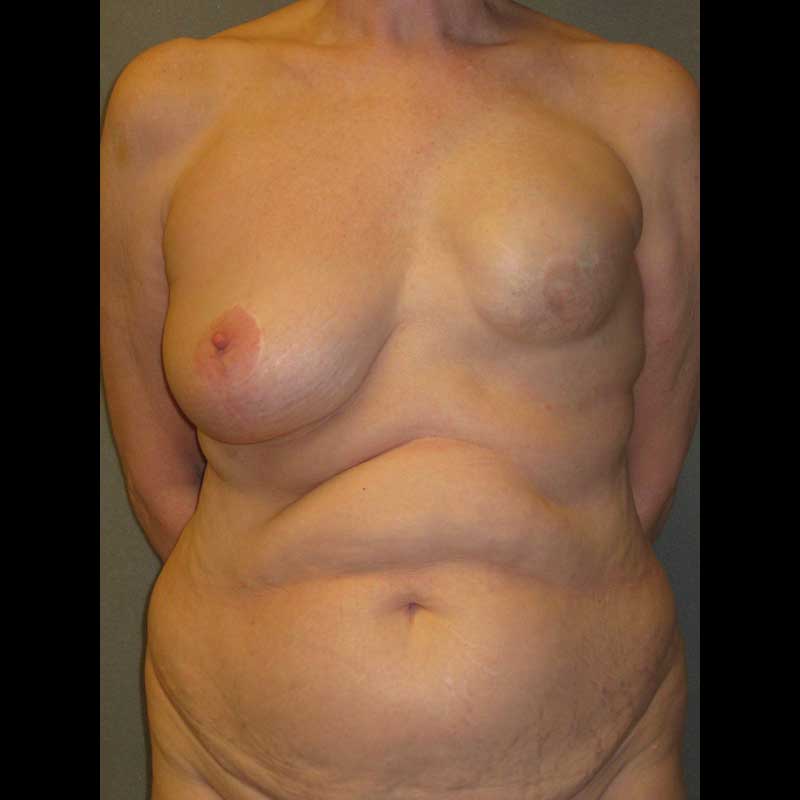
This technique involves removing a flap of skin and fat from the lower abdomen to create a breast. Using perforator surgery and microsurgery techniques, blood vessels are included with the flap, which is then transplanted to the chest wall.
Before surgery, a CT angiogram can help confirm that sufficient blood vessels are present in the lower abdomen. The small blood vessels to the flap are exposed and the flap is transferred to the mastectomy site at the time of the surgery. Using an operating microscope, the flap blood vessels are then connected to blood vessels in the chest. This provides living tissue which can be formed to create a breast shape.
Patients with sufficient lower abdominal skin and fat are good candidates for DIEP/SIEA flap breast reconstruction. This approach is ideal for women who prefer to avoid breast implants. It is also the preferred approach for women that may be poor candidates for implants, such as those women who have previously undergone radiation treatment.
Types of procedures
- DIEP flap: The deep inferior epigastric perforator vessels which pierce the rectus muscle provide the blood supply to this flap. Perforator surgery techniques allow these vessels to be teased out of the rectus muscle while preserving muscle function.
- SIEA flap: In rare cases, the superficial inferior epigastric vessels are available and are large enough to be connected to the vessels in the chest. The SIEA flap avoids deep incisions through muscle, allowing for an easier post-operative recovery.
- TRAM free flap: If the DIEP or SIEA vessels are not ideal, a small portion of rectus muscle may be needed to carry the blood supply of the lower abdominal wall tissue. This is a transverse rectus abdominis myocutaneous free flap.
Procedure details
- CT angiogram before surgery maps the lower abdominal vessels and helps predict which vessels can be used for the flap
- Large ellipse of skin and fat is removed from the lower abdomen at which time vessels needed to support the flap are selected and the flap is transplanted to the chest
- Using microsurgery techniques, blood vessels are connected
- Breast shape is created using the transplanted flap tissue
- After flap transfer, any incisions in the rectus muscle are repaired and the abdomen is closed much like a tummy tuck
Risks & Benefits
In very rare cases, there can be problems with the blood supply to these flaps after surgery. If this occurs, it is possible that the flap tissue does not survive and a different approach to breast reconstruction would be required.
The team of surgeons at NYBRA Plastic Surgery has performed thousands of successful DIEP flap breast reconstructions with a risk of flap loss of less than one percent. Despite this very low risk, we carefully monitor the flap blood supply during the patient’s hospital stay. With Enhanced Recovery After Surgery (ERAS) protocols for all of our DIEP flap patients, the typical hospital stay is two to three days.
After discharge from the hospital, patients are instructed to avoid heavy lifting or exercise for the first few weeks until their abdomen has healed. This is to minimize the risk of hernia or bulging. In the unusual case that a hernia develops, corrective surgery may be recommended.
The primary advantage of DIEP flap breast reconstruction is that it provides for a natural-tissue breast reconstruction while avoiding the need for a breast implant. In addition, many patients appreciate the flatter contour of their lower abdomen.
Frequently Asked Questions
Can I have DIEP flap breast reconstruction if I had previous surgery on my abdomen?
This depends on what surgery you had in the past. A DIEP flap would most likely not be possible if you have had a tummy tuck. However, most other abdominal scars from previous surgery will not interfere with having a DIEP flap. The CT angiogram before surgery can help make this determination.
What will my reconstructed breast feel like?
While the skin will be numb at first, some sensation usually returns over time. Sometimes a sensory nerve in the flap can be used to help restore sensation to the reconstructed breast. In either case, the reconstructed breast will feel soft and warm like a natural breast.