Summary
This flap is typically used as a pedicled or attached flap. Unlike free flaps that are transplanted from one part of the body to another, the blood vessels in a TAP flap remain connected to the body. Once the skin and fat is isolated on the back, the flap is rotated from the back towards the breast.
The TAP flap is most commonly used to reconstruct partial breast or lumpectomy defects. For patients with a small breast size, this flap may provide enough tissue to restore an entire breast following mastectomy. On occasion, the TAP flap may be combined with an implant to add volume.
Procedure details
- Skin and fat used is similar to the LD flap, but without the need to reposition any muscle
- Blood supply comes from small vessels that pierce through the LD muscle on the back
- These perforator vessels are exposed and included with the flap, which is then rotated from the back to the breast
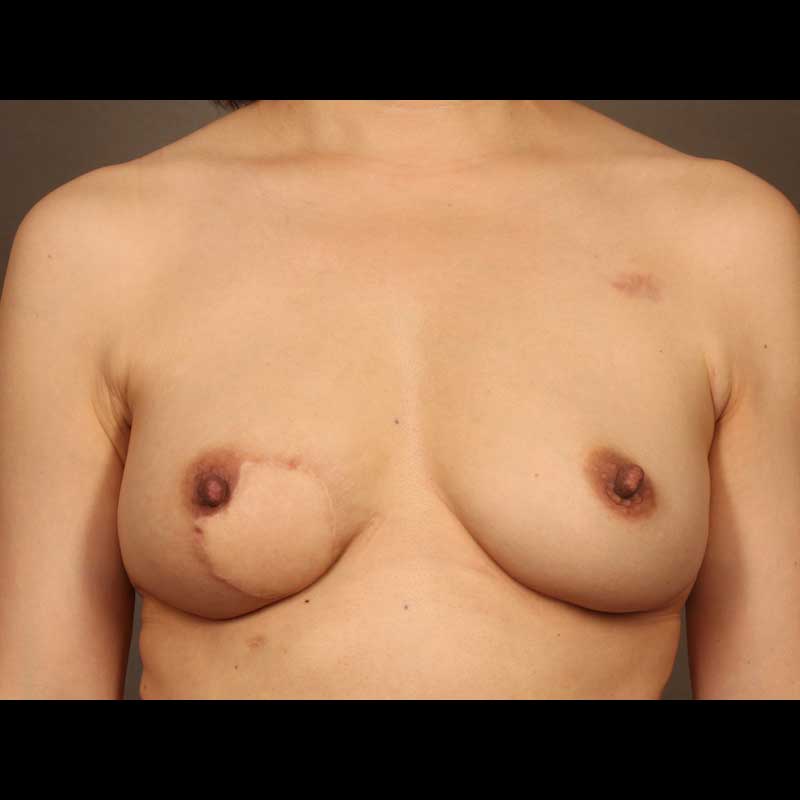
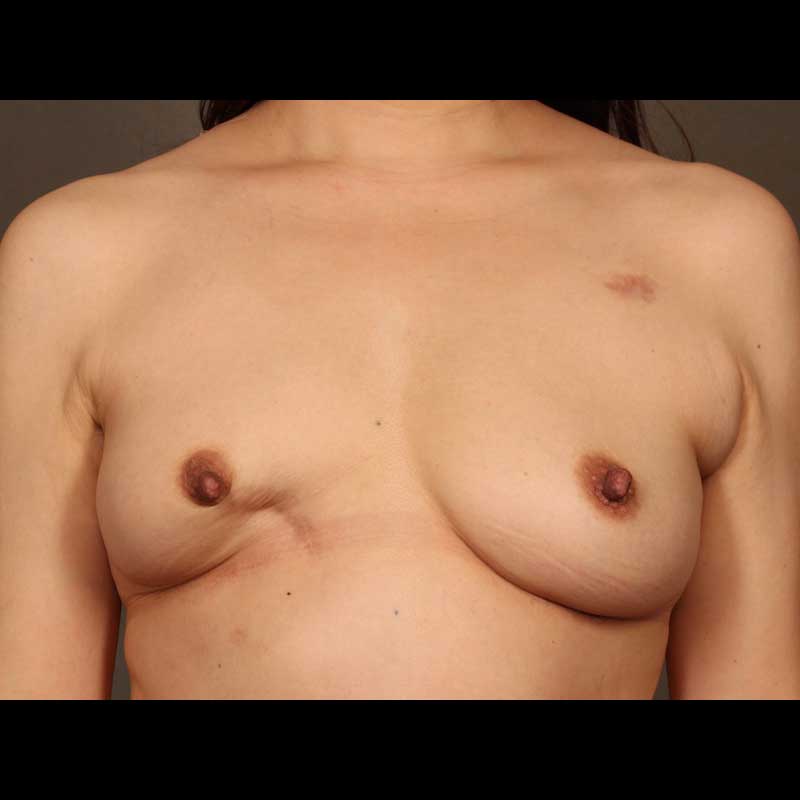
- Skin and fat of the flap can restore natural contour by replacing a defect in the breast
Risks & Benefits
Compared to the latissimus dorsi flap, the TAP flap has some limitations. Only a relatively small amount of tissue can typically be transferred with this flap, which limits the volume available to reconstruct the breast. For this reason the TAP flap is mainly used for partial breast reconstruction or for the correction of lumpectomy defects. Since the latissimus muscle is preserved with this flap, the recovery from surgery is easier.
Frequently Asked Questions
What scars can I expect from this procedure?
The scar on the back is very similar to that of a latissimus dorsi flap. Depending on the size of the flap and on the patient’s anatomy, the scar on the back may be horizontal, vertical, or diagonal.
Will I need drains even though the muscle isn’t removed from my back?
As with other flaps, drains are used for TAP flap breast reconstruction, and are usually removed within one to two weeks.